CagriSema Superior to Semaglutide for HbA1c, Weight Loss in T2D
In a landmark phase 3 trial, CagriSema demonstrated superiority over semaglutide for both HbA1c reduction and weight loss in patients with type 2 diabetes (T2D). Topline results from the REIMAGINE 2 trial highlight the potential of this fixed-dose combination therapy to address key challenges in T2D management: glycemic control and excess body weight.
What is CagriSema and How Does It Work?
CagriSema is a fixed-dose combination of cagrilintide, a long-acting amylin analogue, and semaglutide, a glucagon-like peptide-1 receptor agonist (GLP-1RA). Amylin is a hormone co-secreted with insulin that helps regulate blood glucose by slowing gastric emptying and promoting satiety. Semaglutide, the active ingredient in drugs like Ozempic and Wegovy, mimics GLP-1 to enhance insulin secretion, suppress glucagon, and reduce appetite.
By combining these mechanisms, CagriSema targets multiple pathways involved in glucose homeostasis and energy balance. This dual action is particularly relevant for T2D patients, where insulin resistance, hyperglycemia, and obesity often coexist. In clinical practice, achieving both HbA1c targets below 7% (per ADA guidelines) and meaningful weight loss can reduce cardiovascular risk and improve quality of life.
Overview of the REIMAGINE 2 Trial
The REIMAGINE 2 trial (ClinicalTrials.gov Identifier: NCT06065540) evaluated the efficacy and safety of CagriSema in 2728 adults with T2D inadequately controlled on metformin with or without a sodium-glucose cotransporter 2 inhibitor (SGLT2i). Approximately 40% of participants were using an SGLT2i prior to randomization. Mean baseline HbA1c was 8.2%, and mean baseline body weight was 101 kg—reflecting a population with moderate hyperglycemia and obesity.
Study Design
Participants were randomly assigned to receive subcutaneous injections once weekly for 68 weeks of:
- CagriSema at fixed-dose combinations of 2.4mg/2.4mg or 1.0mg/1.0mg
- Semaglutide monotherapy (2.4mg or 1.0mg)
- Cagrilintide monotherapy (2.4mg)
- Matching placebo
The primary endpoint was the change from baseline in HbA1c at week 68.
Baseline Characteristics and Patient Relevance
This trial mirrors real-world T2D management, where metformin is first-line therapy, often combined with SGLT2is for cardiorenal protection. Patients with HbA1c around 8.2% represent those needing escalation beyond oral agents. Obesity (mean BMI implied by 101 kg weight) is common, affecting over 90% of T2D cases, making weight loss a critical outcome.
Detailed Efficacy Results: HbA1c and Weight Loss
Findings based on the efficacy estimand (assuming full adherence to the study intervention) showed treatment with CagriSema 2.4mg/2.4mg resulted in a statistically significant reduction in HbA1c compared with semaglutide 2.4mg at week 68 (-1.91% points vs -1.76% points).
HbA1c Reductions Across Estimands
Under the treatment regimen estimand (regardless of adherence), CagriSema 2.4mg/2.4mg-treated patients experienced an HbA1c reduction of 1.80% points compared with 1.68% points with semaglutide 2.4mg. These differences, though modest in absolute terms, are clinically meaningful, potentially helping more patients reach ADA targets and reducing complication risks like neuropathy or retinopathy.
Precision tracking for your journey
Join thousands using Shotlee to accurately track GLP-1 medications and side effects.
📱 Get the Shotlee App
Track your GLP-1 medications, peptides, and health metrics on the go with our mobile app!
Weight Loss Outcomes
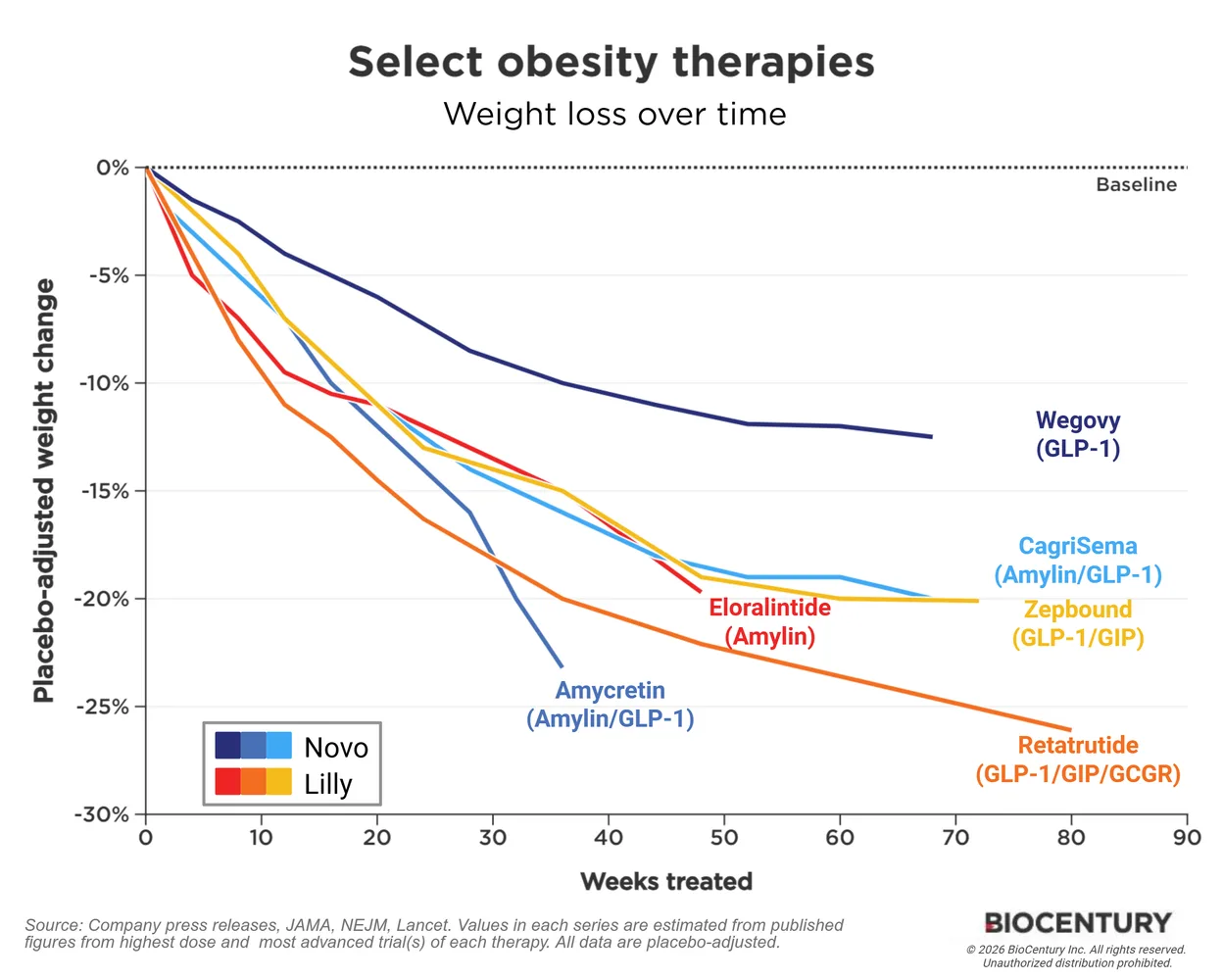
Patients treated with CagriSema 2.4mg/2.4mg achieved a weight loss of 14.2% compared with 10.2% with semaglutide 2.4mg at week 68. No weight loss plateau was noted for CagriSema at the end of the trial. In the CagriSema 2.4mg/2.4mg group, 43% of patients achieved weight loss of at least 15%, while 24% achieved weight loss of at least 20%.
Under the treatment regimen estimand, superior weight loss with CagriSema 2.4mg/2.4mg was also observed (-12.9% vs -9.2% with semaglutide 2.4mg). Sustained weight loss without plateauing suggests ongoing efficacy, unlike some GLP-1RAs where regain occurs post-treatment.
In context, semaglutide 2.4mg already offers robust weight loss (e.g., 15-17% in obesity trials), so CagriSema's edge positions it as a potential next-generation option for T2D patients struggling with weight.
Safety Profile of CagriSema
Gastrointestinal adverse events were reported with CagriSema though they were mild to moderate in intensity and diminished over time. The combination treatment was generally well tolerated, aligning with the known profile of GLP-1RAs and amylin analogues. Common GI effects like nausea typically peak during dose escalation and resolve, supporting once-weekly dosing feasibility.
For patients, this tolerability is key when considering long-term adherence in T2D, where therapy often spans decades.
Expert Commentary
"We are very pleased by the clinical profile of CagriSema in type 2 diabetes patients, including a confirmation of the very strong weight loss data seen with CagriSema in the obesity trials," said Martin Holst Lange, executive vice president, chief scientific officer and head of Research and Development at Novo Nordisk. "By combining semaglutide and cagrilintide, we're seeing superior outcomes in both blood glucose control and weight reduction beyond those achieved with each therapy individually."
Future Implications and Regulatory Status
Full results from REIMAGINE 2 will be presented at a future scientific conference this year. In December 2025, Novo Nordisk submitted an application for CagriSema for weight management to the Food and Drug Administration based on data from the REDEFINE 1 and REDEFINE 2 clinical trials. Approval for T2D could follow, expanding options beyond current GLP-1RAs like semaglutide or tirzepatide.
What This Means for Patients with Type 2 Diabetes
If you're managing T2D on metformin with suboptimal HbA1c or weight, discuss CagriSema with your endocrinologist once approved. It may offer better dual benefits than semaglutide alone, especially if weight loss is a goal. Start with baseline assessments (HbA1c, weight, GI tolerance) and monitor progress. Tools like Shotlee can help track symptoms, side effects, or medication schedules during escalation.
Compare to alternatives: Semaglutide improves CV outcomes (per SELECT trial), but CagriSema's added weight loss could amplify this. Always weigh against lifestyle interventions and SGLT2i combos.
Key Takeaways
- CagriSema 2.4mg/2.4mg superior to semaglutide 2.4mg: HbA1c -1.91% vs -1.76% (efficacy estimand).
- Weight loss: 14.2% vs 10.2%; 43% achieved ≥15% loss.
- Well-tolerated with transient GI events.
- REIMAGINE 2: 2728 T2D patients on metformin ± SGLT2i.
- Potential game-changer for T2D glycemic and weight management.
Conclusion: Actionable Insights
The REIMAGINE 2 trial underscores CagriSema's superiority to semaglutide in T2D, offering deeper HbA1c reductions and greater weight loss. Patients and providers should monitor upcoming full data and approvals. Consult your doctor to see if emerging therapies like this fit your regimen—personalized T2D care starts with evidence-based options. For related topics, explore GLP-1RA comparisons or peptide therapy advances.